Thalitone: Package Insert / Prescribing Info
Package insert / product label
Generic name: chlorthalidone
Dosage form: tablet
Drug class: Thiazide diuretics
Medically reviewed by Drugs.com. Last updated on Jun 14, 2024.
The Thalitone brand name has been discontinued in the U.S. If generic versions of this product have been approved by the FDA, there may be generic equivalents available.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Overdosage
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- How Supplied/Storage and Handling
- Patient Counseling Information
Highlights of Prescribing Information
THALITONE (chlorthalidone) tablets, for oral use
Initial U.S. Approval: 1988
Indications and Usage for Thalitone
THALITONE is a thiazide-like diuretic indicated:
• For the treatment of hypertension, to lower blood pressure. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions (1.1).
• as adjunctive therapy in edema associated with heart failure, cirrhosis of the liver, and renal disease, including nephrotic syndrome (1.2). (1)
Thalitone Dosage and Administration
• Initiate therapy with the lowest possible dose, then titrate according to individual patient response (2.1).
• Hypertension: Recommended initial dose is 15 mg daily with food. If additional blood pressure reduction is needed, increase the dose to 25 mg (2.2).
• Edema: Recommended initial dose is 50 mg to 100 mg daily or 100 mg on alternate days. Depending on response, dosage can be decreased or increased up to a maximum of 200 mg daily (2.3). (2)
Dosage Forms and Strengths
Tablets: 15 mg and 25 mg (3). (3)
Contraindications
• Anuria (4).
• Hypersensitivity (4). (4)
Warnings and Precautions
• Hypotension: Higher risk for patients with impaired sympathetic response, volume-depletion or salt restriction (5.1).
• Renal Impairment: Patients with pre-existing kidney disease may be at higher risk. (5.2).
• Monitor serum electrolytes periodically (5.3). (5)
Adverse Reactions/Side Effects
The most frequently expected adverse drug reactions among patients receiving THALITONE are hypotension, dizziness, renal dysfunction, and electrolyte abnormalities (6).
To report SUSPECTED ADVERSE REACTIONS, contact Casper Pharma LLC at 1-844-5-CASPER (1-844-522-7737) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. (6)
Drug Interactions
• Antihypertensive drugs: Chlorthalidone may add to or potentiate the action of other antihypertensive drugs (7).
• Lithium: Lithium renal clearance is reduced by chlorthalidone, increasing the risk of lithium toxicity (7). (7)
Use In Specific Populations
• Pregnancy: May cause fetal harm (8.1).
• Lactation: Breastfeeding not recommended (8.2).
• Pediatrics: Safety and efficacy in children have not been established (8.4).
• Geriatric Use: No overall difference in responses versus younger patients but care should be taken in dose selection in patients with impaired renal function (8.5). (8)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2021
Full Prescribing Information
1. Indications and Usage for Thalitone
1.1 Hypertension
THALITONE® is indicated for the treatment of hypertension, to lower blood pressure. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. These benefits have been seen in controlled trials of antihypertensive drugs from a wide variety of pharmacologic classes including the class to which this drug principally belongs. There are no controlled trials demonstrating risk reduction with THALITONE.
Control of high blood pressure should be part of comprehensive cardiovascular risk management, including, as appropriate, lipid control, diabetes management, antithrombotic therapy, smoking cessation, exercise, and limited sodium intake. Many patients will require more than one drug to achieve blood pressure goals. For specific advice on goals and management, see published guidelines, such as those of the National High Blood Pressure Education Program’s Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC).
Numerous antihypertensive drugs, from a variety of pharmacologic classes and with different mechanisms of action, have been shown in randomized controlled trials to reduce cardiovascular morbidity and mortality, and it can be concluded that it is blood pressure reduction, and not some other pharmacologic property of the drugs, that is largely responsible for those benefits. The largest and most consistent cardiovascular outcome benefit has been a reduction in the risk of stroke, but reductions in myocardial infarction and cardiovascular mortality also have been seen regularly.
Elevated systolic or diastolic pressure causes increased cardiovascular risk, and the absolute risk increase per mmHg is greater at higher blood pressures, so that even modest reductions of severe hypertension can provide substantial benefit. Relative risk reduction from blood pressure reduction is similar across populations with varying absolute risk, so the absolute benefit is greater in patients who are at higher risk independent of their hypertension (for example, patients with diabetes or hyperlipidemia), and such patients would be expected to benefit from more aggressive treatment to a lower blood pressure goal.
THALITONE can be used alone or in combination with other antihypertensive agents.
2. Thalitone Dosage and Administration
2.1 General Considerations
THALITONE cannot be substituted with other formulations of chlorthalidone.
Initiate therapy with the lowest possible dose, then titrate according to individual patient response.
3. Dosage Forms and Strengths
THALITONE 15 mg tablets are white biconvex, kidney shaped tablets with “L” on lower punch and “96” on the upper punch.
THALITONE 25 mg tablets are white biconvex, kidney shaped tablets with “L” on one side and “99” on the other side.
4. Contraindications
THALITONE is contraindicated in patients with anuria or hypersensitivity to chlorthalidone or other sulfonamide-derived drugs.
5. Warnings and Precautions
5.1 Hypotension
THALITONE may cause symptomatic hypotension. Patients with impaired sympathetic response, volume-depletion or who are salt restricted may be at increased risk for developing hypotension.
If hypotension occurs, place the patient in the supine position and, if necessary, give intravenous normal saline. A transient hypotensive response is not a contraindication to further treatment, which usually can be continued without difficulty once the blood pressure has stabilized.
5.2 Impaired Renal Function
Changes in renal function including acute renal failure can be caused by diuretics. Patients with chronic kidney disease, heart failure, or volume depletion may be at particular risk of developing acute renal failure on THALITONE. Monitor renal function periodically. Consider withholding or discontinuing therapy in patients who develop a clinically significant decrease in renal function on THALITONE [see Drug Interactions (7)].
5.3 Electrolyte Abnormalities
THALITONE can cause hypokalemia, hyponatremia, hypochloremic alkalosis, and hypomagnesemia. Hypomagnesemia can result in hypokalemia which appears difficult to treat despite potassium repletion. Monitor serum electrolytes periodically.
If hypokalemia is accompanied by clinical signs (e.g., muscular weakness, paresis, or ECG alterations), THALITONE should be discontinued. Correction of hypokalemia and any coexisting hypomagnesemia is recommended prior to the initiation of thiazides.
5.4 Metabolic Disturbances
Chlorthalidone may alter glucose tolerance.
Chlorthalidone may raise serum levels of cholesterol and triglycerides.
Chlorthalidone may raise the serum uric acid level due to reduced clearance of uric acid and may cause or exacerbate hyperuricemia and precipitate gout in susceptible patients.
Chlorthalidone decreases urinary calcium excretion and may cause elevations of serum calcium. Monitor calcium levels in patients with hypercalcemia receiving THALITONE.
6. Adverse Reactions/Side Effects
The following adverse reactions are described in more detail elsewhere in the label;
• Hypotension [see Warnings and Precautions (5.1)]
• Impaired Renal Function [see Warnings and Precautions (5.2)]
• Electrolyte Abnormalities [see Warnings and Precautions (5.3)]
• Metabolic Disturbances [see Warnings and Precautions (5.4)]
The following adverse reactions have been observed, but there is not enough systematic collection of data to support an estimate of their frequency.
Gastrointestinal System Reactions: anorexia, gastric irritation, nausea, vomiting, cramping, diarrhea, constipation, jaundice (intrahepatic cholestatic jaundice), pancreatitis.
Central Nervous System Reactions: dizziness, paresthesias, headache.
Hematologic Reactions: leukopenia, agranulocytosis, thrombocytopenia, aplastic anemia.
Dermatologic-Hypersensitivity Reactions: purpura, photosensitivity, rash, urticaria, necrotizing angiitis (vasculitis) (cutaneous vasculitis), Lyell’s syndrome (toxic epidermal necrolysis).
Cardiovascular Reaction: Orthostatic hypotension.
Other Adverse Reactions: muscle spasm, weakness, restlessness, impotence, xanthopsia.
7. Drug Interactions
Effect of chlorthalidone on other drugs
Chlorthalidone may add to or potentiate the action of other antihypertensive drugs.
Chlorthalidone and related drugs may increase the responsiveness to tubocurarine.
Lithium renal clearance is reduced by chlorthalidone, increasing the risk of lithium toxicity. Monitor serum lithium levels during concomitant use.
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
Available data over decades from observational studies and reports with chlorthalidone use in pregnant women have not identified a drug-associated risk of major birth defects or miscarriage. However, adverse fetal outcomes, including fetal or neonatal jaundice, thrombocytopenia, hypoglycemia, and electrolyte abnormalities have been reported following maternal use of thiazide diuretics (see Clinical Considerations). Chlorthalidone should not be used as first-line therapy to treat hypertension in pregnancy. Advise pregnant women of the potential risk to a fetus.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risks of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
Hypertension in pregnancy increases the maternal risk for pre-eclampsia, gestational diabetes, premature delivery, and delivery complications (e.g., need for cesarean section, and post-partum hemorrhage). Hypertension increases the fetal risk for intrauterine growth restriction and stillbirth.
Fetal/Neonatal Adverse Reactions
Thiazides can cross the placenta, and concentrations reached in the umbilical vein approach those in the maternal plasma. Thiazides, like other diuretics, can cause placental hypoperfusion. Use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice, thrombocytopenia, hypoglycemia, and electrolyte abnormalities. Thiazides do not prevent or alter the course of EPH (Edema, Proteinuria, Hypertension) gestosis (pre-eclampsia) and should not be used as first-line therapy to treat hypertension in pregnant women.
Data
Animal Data
Reproduction studies have been performed in the rat and the rabbit and have revealed no evidence of harm to the fetus due to chlorthalidone.The available data do not allow the calculation of comparisons between the exposure of chlorthalidone observed in animal studies to the systemic exposure that would be expected in humans.
8.2 Lactation
Risk Summary
Chlorthalidone is present in human milk. There is no information regarding the effects of chlorthalidone on the breastfed infant or the effects on milk production. Because of the potential for chlorthalidone accumulation which may lead to serious adverse reactions in the breastfed infant (such as jaundice, thrombocytopenia, hyperglycemia, electrolyte abnormalities), advise patients that breastfeeding is not recommended during treatment with chlorthalidone.
8.5 Geriatric Use
Clinical studies of THALITONE did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function, and of concomitant disease or other drug therapy.
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
10. Overdosage
Symptoms of acute overdosage include nausea, weakness, dizziness and disturbances of electrolyte balance. The oral LD50 of the drug in the mouse and the rat is more than 25,000 mg/kg body weight. The minimum lethal dose (MLD) in humans has not been established. There is no specific antidote but gastric lavage is recommended, followed by supportive treatment. Where necessary, this may include intravenous dextrose-saline with potassium, administered with caution.
11. Thalitone Description
THALITONE (chlorthalidone USP) is an antihypertensive/diuretic supplied as 15 mg and 25 mg tablets for oral use. It is a monosulfamyl diuretic that differs chemically from thiazide diuretics in that a double ring system is incorporated in its structure. It is a racemic mixture of 2-chloro-5-(1-hydroxy-3-oxo-1-isoindolinyl) benzenesulfonamide, with the following structural formula:
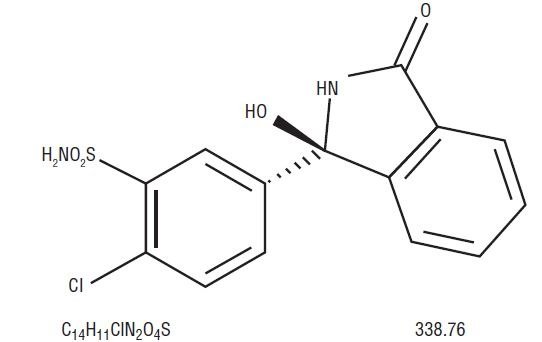
Chlorthalidone is practically insoluble in water, in ether and in chloroform; soluble in methanol; slightly soluble in alcohol.
The inactive ingredients are colloidal silicon dioxide, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, sodium starch glycolate.
12. Thalitone - Clinical Pharmacology
12.1 Mechanism of Action
Chlorthalidone is a long-acting oral diuretic with antihypertensive activity. The diuretic effects of chlorthalidone and the benzothiadiazine (thiazide) diuretics appear to arise from similar mechanisms and the maximal effect of chlorthalidone and the thiazides appear to be similar. The site of the action appears to be the distal convoluted tubule of the nephron. Although the mechanism of action of chlorthalidone and related drugs is not wholly clear, sodium and water depletion appear to provide a basis for its antihypertensive effect.
12.2 Pharmacodynamics
The diuretic action of chlorthalidone commences a mean of 2.6 hours after dosing and continues for up to 72 hours. The drug produces diuresis with increased excretion of sodium and chloride. The diuretic effects of chlorthalidone lead to decreased extracellular fluid volume, plasma volume, cardiac output, total exchangeable sodium, glomerular filtration rate, and renal plasma flow. Chlorthalidone produces dose-related reductions in serum potassium levels, elevations in serum uric acid and blood glucose, and it can lead to decreased sodium and chloride levels.
12.3 Pharmacokinetics
Absorption
THALITONE (chlorthalidone USP) has been formulated with PVP (povidone polyvinylpyrrolidone), a bioavailability enhancer that provides 104% to 116% bioavailability relative to an oral solution of chlorthalidone [see Clinical Studies (14)]. THALITONE cannot be substituted with other formulations of chlorthalidone.
Distribution
In the blood, approximately 75% of the drug is bound to plasma proteins over a concentration range of 0.2 to 7.7 ug/mL.
Elimination
The mean plasma half-life of chlorthalidone is about 40 to 60 hours. It is eliminated primarily as unchanged drug in the urine.
14. Clinical Studies
Two similarly designed, 12-week, double-blind, parallel group, placebo-controlled multicenter studies were conducted to compare THALITONE 15 mg to the standard chlorthalidone 25 mg in terms of reduction in blood pressure and metabolic disturbances. Collectively, a total of 222 patients with long-standing diastolic blood pressure between 90 and 104 mm Hg were randomized to receive THALITONE 15 mg (N=71), standard chlorthalidone 25 mg (N=75), or placebo (N=76).
THALITONE 15 mg has the advantage of demonstrating potentially fewer metabolic disturbances (Table 1) in particular, lowered glucose levels when compared to Hygroton® 25 mg in clinical setting (Table 2). THALITONE 15 mg helps meet the goal of lowering blood pressure in patients that respond to Chlorthalidone therapy. In general, electrolyte abnormalities are a class effect associated with Chlorthalidone therapy.
Table 1. Reduction in blood pressure at 12 weeks (THALITONE 15 mg vs. Standard chlorthalidone 25 mg)
| Pairwise comparison
| 2 through 12 weeks
| 4 through 12 weeks
|
||
|---|---|---|---|---|
| Mean change (95% CI)
| Significance level
| Mean change
(95% CI) | Significance level
|
|
| Standing SBP, mm Hg
|
||||
| THALITONE 15 mg vs. placebo | −11.77 vs. −1.89 (−13.02, −6.74) | <0.001 | −12.43 vs. −2.02 (−13.87, −6.95) | <0.001 |
| THALITONE 15 mg vs. standard chlorthalidone 25 mg | −11.77 vs. −11.73 (−3.18, 3.1) | 0.98 | −12.43 vs. −11.70 (−4.19, 2.73) | 0.68 |
| Standing DBP, mm Hg
|
||||
| THALITONE 15 mg vs. placebo | −5.95 vs. −3.28 (−4.5, −0.84) | <0.01 | −6.64 vs. −3.42 (−5.29, −1.15) | <0.01 |
| THALITONE 15 mg vs. standard chlorthalidone 25 mg | − 5.95 vs. −6.79 (−0.99, 2.67) | 0.37 | −6.64 vs. −7.06 (−1.65, 2.49) | 0.69 |
| Supine SBP, mm Hg
|
||||
| THALITONE 15 mg vs. placebo | −8.42 vs. −2.63 (−8.87, −2.71) | <0.001 | −8.91 vs. −2.85 (-9.46, -2.66) | <0.001 |
| THALITONE 15 mg vs. standard chlorthalidone 25 mg | −8.42 vs. −10.31 (−1.19, 4.97) | 0.23 | −8.91 vs. −10.61 (−1.70, 5.10) | 0.33 |
| Supine DBP, mm Hg
|
||||
| THALITONE 15 mg vs. placebo | −6.44 vs. −4.16 (−4.46, −0.11) | 0.04 | −6.72 vs. −4.28 (−4.85, −0.03) | 0.05 |
| THALITONE 15 mg vs. standard chlorthalidone 25 mg | −6.44 vs. −6.82 (−1.80, 2.56) | 0.73 | −6.72 vs. −7.05 (−2.08, 2.74) | 0.79 |
SBP: systolic blood pressure, DBP: diastolic blood pressure, CI: confidence interval
Table 2. Mean changes in laboratory parameters (THALITONE 15 mg vs. Standard chlorthalidone 25 mg)
| Parameter
| THALITONE 15 mg
| Standard chlorthalidone 25 mg
| Placebo
|
|
|---|---|---|---|---|
| Potassium (mmol/L)
|
||||
| Baseline | N/A | N/A | N/A |
|
| 4 Weeks | −0.35 (0.08)* | −0.53 (0.05)* | 0.10 (0.05) |
|
| 12 Weeks | −0.31 (0.07)* | −0.55 (0.06)* | 0.12 (0.06) |
|
| Cholesterol (mg/dL)
|
||||
| Baseline | N/A | N/A | N/A |
|
| 4 Weeks | 5.51 (3.70)* | 5.14 (3.29)* | −7.18 (3.30) |
|
| 12 Weeks | 9.34 (3.03) | 8.11 (3.86) | 0.26 (4.53) |
|
| Glucose (mg/dL)
|
||||
| Baseline | N/A | N/A | N/A |
|
| 4 Weeks | 1.83 (2.55) | 6.56 (2.36) | 1.52 (2.17) |
|
| 12 Weeks | −0.84 (2.58)+
| 11.02 (2.71)* | −1.83 (2.29) |
|
| Uric Acid (mg/dL)
|
||||
| Baseline | N/A | N/A | N/A |
|
| 4 Weeks | 0.66 (0.16)* | 1.04 (0.14)* | −0.34 (0.15) |
|
| 12 Weeks | 0.71 (0.13)* | 1.10 (0.14)* | −0.19 (0.15) |
|
*p<0.05 vs. placebo
+p<0.05 vs. standard chlorthalidone 25 mg
N/A: Not Applicable
16. How is Thalitone supplied
THALITONE (chlorthalidone) Tablets USP 15 mg are white biconvex, kidney shaped tablets with “L” on lower punch and “96” on the upper punch.
Bottles of 30 NDC 70199-017-30
Bottles of 100 NDC 70199-017-01
THALITONE (chlorthalidone) Tablets USP 25 mg are white biconvex, kidney shaped tablets with “L” on one side and “99” on the other side.
Bottles of 30 NDC 70199-001-30
Bottles of 100 NDC 70199-001-01
Store at 20o to 25oC (68o to 77oF). [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP using a child-resistant closure.
17. Patient Counseling Information
• Patients should inform their doctor if they have had an allergic reaction to chlorthalidone or other diuretics; kidney disease; gout; been taking lithium carbonate.
• Patients should be cautioned to contact their physician if they experience any of the following symptoms of potassium loss: excess thirst, tiredness, drowsiness, restlessness, muscle pains or cramps, nausea, vomiting or increased heart rate or pulse.
• Patients should inform their doctor if they have symptoms of light-headedness or dizziness.
• Pregnancy
Advise a pregnant woman of the potential risk to a fetus. Advise females of reproductive potential to inform their prescriber of a known or suspected pregnancy [see Use in Specific Populations (8.1)].
• Lactation
Advise females not to breastfeed during treatment with chlorthalidone [see Use in Specific Populations (8.2)].
Rx Only
PIB00101-05
Manufactured for:
Casper Pharma LLC
East Brunswick, NJ 08816
Made in India.
Revised: 12/2019
| THALITONE
chlorthalidone tablet |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| THALITONE
chlorthalidone tablet |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Casper Pharma LLC (080025838) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Aurobindo Pharma Limited | 650381903 | ANALYSIS(70199-001, 70199-017) , MANUFACTURE(70199-001, 70199-017) , PACK(70199-001, 70199-017) | |
Frequently asked questions
More about Thalitone (chlorthalidone)
- Check interactions
- Compare alternatives
- Pricing & coupons
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Drug class: thiazide diuretics
- Breastfeeding
