Horizant: Package Insert / Prescribing Info
Package insert / product label
Generic name: gabapentin enacarbil
Dosage form: tablet, extended release
Drug class: Gamma-aminobutyric acid analogs
Medically reviewed by Drugs.com. Last updated on Sep 1, 2023.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Drug Abuse and Dependence
- Overdosage
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- How Supplied/Storage and Handling
- Storage and Handling
- Patient Counseling Information
- Medication Guide
Highlights of Prescribing Information
HORIZANT® (gabapentin enacarbil) Extended-Release Tablets for oral use
Initial U.S. Approval: 2011
Indications and Usage for Horizant
Horizant Dosage and Administration
Instruct patients to swallow tablets whole and not to cut, crush, or chew tablets. Take with food. (2)
RLS: 600 mg once daily taken at about 5 PM. (2.1)
- A dose of 1,200 mg once daily provided no additional benefit compared with the 600-mg dose, but caused an increase in adverse reactions. (2.1)
- If the dose is not taken at the recommended time, the next dose should be taken the following day as prescribed. (2.1)
PHN: The starting dose is 600 mg in the morning for 3 days, then increase to 600 mg twice daily beginning on day 4. (2.2)
- A daily dose greater than 1,200 mg provided no additional benefit. (2.2)
- If the dose is not taken at the recommended time, skip this dose, and the next dose should be taken at the time of next scheduled dose. (2.2)
Patients with renal impairment: Doses of HORIZANT must be adjusted in accordance with renal function. (2.3)
Dosage Forms and Strengths
Extended-Release Tablets: 300 mg and 600 mg. (3)
Contraindications
None. (4)
Warnings and Precautions
- Driving impairment: Warn patients not to drive until they have gained sufficient experience with HORIZANT to assess whether it will impair their ability to drive. (5.1)
- Somnolence/sedation and dizziness: May impair the patient's ability to operate complex machinery. (5.2)
- HORIZANT is not interchangeable with other gabapentin products. (5.3)
- Suicidal thoughts or behaviors: HORIZANT is a prodrug of gabapentin, an antiepileptic drug (AED). AEDs increase the risk of suicidal thoughts or behaviors. Monitor for suicidal thoughts or behaviors. (5.4)
- Respiratory depression: May occur with HORIZANT when used with concomitant central nervous system (CNS) depressants or in the setting of concurrent respiratory impairment. Monitor patients and adjust dosage as appropriate (5.5).
Adverse Reactions/Side Effects
- RLS: Most common adverse reactions (≥10% and at least 2 times the rate of placebo) were somnolence/sedation and dizziness. (6.1)
- PHN: Most common adverse reactions (≥10% and greater than placebo) were dizziness, somnolence, and headache. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Azurity Pharmaceuticals, Inc. at 1-800-461-7449 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 8/2022
Full Prescribing Information
1. Indications and Usage for Horizant
2. Horizant Dosage and Administration
Tablets should be swallowed whole and should not be cut, crushed, or chewed.
Tablets should be taken with food.
HORIZANT is not interchangeable with other gabapentin products because of differing pharmacokinetic profiles [see Warnings and Precautions (5.3)].
2.1 Restless Legs Syndrome
The recommended dosage for HORIZANT is 600 mg once daily at about 5 PM. A daily dose of 1,200 mg provided no additional benefit compared with the 600-mg dose, but caused an increase in adverse reactions [see Adverse Reactions (6.1)].
If the dose is not taken at the recommended time, the next dose should be taken the following day as prescribed.
2.2 Postherpetic Neuralgia
The recommended dosage of HORIZANT is 600 mg twice daily. HORIZANT should be initiated at a dose of 600 mg in the morning for 3 days of therapy, then increased to 600 mg twice daily (1,200 mg/day) on day four. In the 12-week principal efficacy study, additional benefit of using doses greater than 1,200 mg a day was not demonstrated, and these higher doses resulted in an increase in adverse reactions [see Adverse Reactions (6.1)].
If the dose is not taken at the recommended time, skip this dose, and the next dose should be taken at the time of the next scheduled dose.
2.3 Renal Impairment
Dosing of HORIZANT is adjusted in accordance with renal function, as represented by creatinine clearance [see Clinical Pharmacology (12.3)]. Target dose regimens are listed in Table 1 and Table 2.
| Creatinine Clearance (mL/min) | Target Dose Regimen |
|---|---|
| ≥60 | 600 mg per day |
| 30 – 59 | Start at 300 mg per day and increase to 600 mg as needed |
| 15 – 29 | 300 mg per day |
| <15 | 300 mg every other day |
| <15 on hemodialysis | Not recommended |
| Creatinine Clearance (mL/min) | Titration | Maintenance | Tapering |
|---|---|---|---|
|
|||
| ≥60 | 600 mg in AM for 3 days | 600 mg twice daily | 600 mg in AM for 1 week |
| 30 – 59 | 300 mg in AM for 3 days | 300 mg twice daily. Increase to 600 mg twice daily as needed* | Reduce current maintenance dose to once daily in AM for 1 week |
| 15 – 29 | 300 mg in AM on Day 1 and Day 3 | 300 mg in AM. Increase to 300 mg twice daily if needed* | If taking 300 mg twice daily, reduce to 300 mg once daily in AM for 1 week. If taking 300 mg once daily, no taper needed. |
| <15 | None | 300 mg every other day in AM. Increase to 300 mg once daily in AM if needed* | None |
| <15 on hemodialysis | None | 300 mg following every dialysis. Increase to 600 mg following every dialysis if needed* | None |
In patients with stable renal function, CrCl can be estimated using the equation of Cockcroft and Gault:
- for males: CrCl = (140-age)(weight)/[(72)(SCr)]
- for females: CrCl = (0.85)(140-age)(weight)/[(72)(SCr)]
where age is in years, weight is in kilograms, and SCr is serum creatinine in mg/dL.
3. Dosage Forms and Strengths
HORIZANT Extended-Release Tablets, 300 mg, are white to off-white, oval-shaped tablets debossed with "GS TF7" and 600 mg, are white to off-white, oval-shaped tablets debossed with "GS LFG". Both the 300 mg and 600 mg tablets may contain occasional black/grey spots.
5. Warnings and Precautions
5.1 Effects on Driving
HORIZANT may cause significant driving impairment [see Clinical Studies (14.3)]. The duration of driving impairment after starting therapy with HORIZANT is unknown. Patients taking HORIZANT should not drive until they have gained sufficient experience to assess whether HORIZANT impairs their ability to drive. However, prescribers and patients should be aware that patients' ability to assess their own driving competence, as well as their ability to assess the degree of somnolence caused by HORIZANT, can be imperfect. Whether the impairment is related to somnolence [see Warnings and Precautions (5.2)] or other effects of HORIZANT is unknown.
5.2 Somnolence/Sedation and Dizziness
HORIZANT causes somnolence/sedation and dizziness (see Tables 4 and 5). Patients should be advised not to drive a car or operate other complex machinery until they have gained sufficient experience on HORIZANT to assess whether HORIZANT impairs their ability to perform these tasks.
During the controlled trials in patients with RLS, somnolence/sedation was reported in 20% of patients treated with 600 mg of HORIZANT per day compared with 6% of patients receiving placebo. In those patients treated with HORIZANT who reported somnolence, the somnolence persisted during treatment in about 30%. In the remaining patients, symptoms resolved within 3 to 4 weeks. Dizziness was reported in 13% of patients receiving 600 mg of HORIZANT per day compared with 4% of patients receiving placebo. In those patients treated with HORIZANT who reported dizziness, symptoms persisted during treatment in about 20%. Somnolence/sedation led to withdrawal in 2% of patients receiving 600 mg of HORIZANT per day. Dizziness led to withdrawal in 1% of patients receiving 600 mg of HORIZANT per day. The incidence of these adverse reactions was greater in the patients receiving 1,200 mg per day.
During the 12-week, controlled study in patients with PHN, somnolence was reported in 10% of patients treated with 1,200 mg of HORIZANT per day compared with 8% of patients receiving placebo. Fatigue/asthenia was reported in 6% of patients treated with 1,200 mg of HORIZANT per day compared with 1% of patients receiving placebo. In those patients treated with 1,200 mg of HORIZANT per day who reported somnolence (10%), the somnolence persisted during treatment in about 27%. In the remaining patients, symptoms resolved within 4 to 5 weeks. Dizziness was reported in 17% of patients receiving 1,200 mg of HORIZANT per day compared with 15% of patients receiving placebo. In those patients treated with 1,200 mg of HORIZANT per day who reported dizziness, symptoms persisted during treatment in about 6%. Somnolence led to withdrawal in <1% of patients receiving 1,200 mg of HORIZANT per day compared with 2% of patients receiving placebo. Dizziness led to withdrawal in 2% of patients receiving 1,200 mg of HORIZANT per day compared with 3% of patients receiving placebo.
5.3 Lack of Interchangeability With Gabapentin
HORIZANT is not interchangeable with other gabapentin products because of differing pharmacokinetic profiles. The same dose of HORIZANT results in different plasma concentrations of gabapentin relative to other gabapentin products [see Clinical Pharmacology (12.3)].
The safety and effectiveness of HORIZANT in patients with epilepsy have not been studied.
5.4 Suicidal Behavior and Ideation
HORIZANT (gabapentin enacarbil) is a prodrug of gabapentin, an antiepileptic drug (AED). AEDs increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Because HORIZANT is a prodrug of gabapentin, HORIZANT also increases this risk. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Pooled analyses of 199 placebo-controlled clinical trials (monotherapy and adjunctive therapy) of 11 different AEDs showed that patients randomized to 1 of the AEDs had approximately twice the risk [adjusted relative risk 1.8, 95% confidence interval (CI): 1.2, 2.7] of suicidal thinking or behavior compared with patients randomized to placebo. In these trials, which had a median treatment duration of 12 weeks, the estimated incidence rate of suicidal behavior or ideation among 27,863 AED-treated patients was 0.43%, compared with 0.24% among 16,029 placebo-treated patients, representing an increase of approximately 1 case of suicidal thinking or behavior for every 530 patients treated. There were 4 suicides in drug-treated patients in the trials and none in placebo-treated patients, but the number is too small to allow any conclusion about drug effect on suicide.
The increased risk of suicidal thoughts or behavior with AEDs was observed as early as 1 week after starting drug treatment with AEDs and persisted for the duration of treatment assessed. Because most trials included in the analysis did not extend beyond 24 weeks, the risk of suicidal thoughts or behavior beyond 24 weeks could not be assessed.
The risk of suicidal thoughts or behavior was generally consistent among drugs in the data analyzed. The finding of increased risk with AEDs of varying mechanisms of action and across a range of indications suggests that the risk applies to all AEDs used for any indication. The risk did not vary substantially by age (5 to 100 years) in the clinical trials analyzed. Table 3 shows absolute and relative risk by indication for all evaluated AEDs.
| Indication | Placebo Patients With Events Per 1,000 Patients | Drug Patients With Events Per 1,000 Patients | Relative Risk: Incidence of Events in Drug Patients/Incidence in Placebo Patients | Risk Difference: Additional Drug Patients With Events Per 1,000 Patients |
|---|---|---|---|---|
| Epilepsy | 1.0 | 3.4 | 3.5 | 2.4 |
| Psychiatric | 5.7 | 8.5 | 1.5 | 2.9 |
| Other | 1.0 | 1.8 | 1.9 | 0.9 |
| Total | 2.4 | 4.3 | 1.8 | 1.9 |
The relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications.
Anyone considering prescribing HORIZANT must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Patients, their caregivers, and families should be informed that HORIZANT increases the risk of suicidal thoughts and behavior and should be advised of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm.
Behaviors of concern should be reported immediately to healthcare providers.
5.5 Respiratory Depression
There is evidence from case reports, human studies, and animal studies associating gabapentin with serious, life-threatening, or fatal respiratory depression when co-administered with central nervous system (CNS) depressants, including opioids, or in the setting of underlying respiratory impairment. When the decision is made to co-prescribe HORIZANT with another CNS depressant, particularly an opioid, or to prescribe HORIZANT to patients with underlying respiratory impairment, monitor patients for symptoms of respiratory depression and sedation, and consider initiating HORIZANT at a low dose. The management of respiratory depression may include close observation, supportive measures, and reduction or withdrawal of CNS depressants (including HORIZANT).
5.6 Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS)/Multiorgan Hypersensitivity
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), also known as multiorgan hypersensitivity, has been reported in patients taking antiepileptic drugs, including gabapentin. HORIZANT is a prodrug of gabapentin. Some of these events have been fatal or life-threatening. DRESS typically, although not exclusively, presents with fever, rash, lymphadenopathy, and/or facial swelling, in association with other organ system involvement, such as hepatitis, nephritis, hematological abnormalities, myocarditis, or myositis sometimes resembling an acute viral infection. Eosinophilia is often present. Because this disorder is variable in its expression, other organ systems not noted here may be involved.
It is important to note that early manifestations of hypersensitivity, such as fever or lymphadenopathy, may be present even though rash is not evident. If such signs or symptoms are present, the patient should be evaluated immediately. HORIZANT should be discontinued if an alternative etiology for the signs or symptoms cannot be established.
5.7 Discontinuation of HORIZANT
When discontinuing HORIZANT, patients with RLS receiving 600 mg or less once daily can discontinue the drug without tapering. If the recommended dose is exceeded, the dose should be reduced to 600 mg daily for 1 week prior to discontinuation to minimize the potential of withdrawal seizure.
In patients with PHN receiving HORIZANT twice daily, the dose should be reduced to once daily for 1 week prior to discontinuation to minimize the potential of withdrawal seizure, see Table 2 [see Dosage and Administration (2.3)].
5.8 Tumorigenic Potential
In an oral carcinogenicity study, gabapentin enacarbil increased the incidence of pancreatic acinar cell adenoma and carcinoma in male and female rats [see Nonclinical Toxicology (13.1)]. The clinical significance of this finding is unknown.
In clinical studies of gabapentin as adjunctive therapy in epilepsy comprising 2,085 patient-years of exposure in patients >12 years of age, new tumors were reported in 10 patients (2 breast, 3 brain, 2 lung, 1 adrenal, 1 non-Hodgkin's lymphoma, 1 endometrial carcinoma in situ), and preexisting tumors worsened in 11 patients (9 brain, 1 breast, 1 prostate) during or up to 2 years following discontinuation of gabapentin. Without knowledge of the background incidence and recurrence in a similar population not treated with gabapentin, it is impossible to know whether the incidence reported in this cohort is or is not affected by treatment.
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions are described in more detail in the Warnings and Precautions section of the label:
- Effects on Driving [see Warnings and Precautions (5.1)]
- Somnolence/Sedation and Dizziness [see Warnings and Precautions (5.2)]
- Suicidal Behavior and Ideation [see Warnings and Precautions (5.4)]
- Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS)/Multiorgan Hypersensitivity[see Warnings and Precautions (5.5)]
- Respiratory Depression [see Warnings and Precautions (5.5)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In all controlled and uncontrolled trials across various patient populations, more than 2,300 patients have received HORIZANT orally in daily doses ranging from 600 to 3,600 mg.
Restless Legs Syndrome
The exposure to HORIZANT in 1,201 patients with RLS included 613 exposed for at least 6 months and 371 exposed for at least 1 year. HORIZANT in the treatment of RLS was studied primarily in placebo-controlled trials (n = 642), and in long- term follow-up studies. The population with RLS ranged from 18 to 82 years of age, with 60% being female and 95% being Caucasian.
The safety of HORIZANT in doses ranging from 600 to 2,400 mg has been evaluated in 515 patients with RLS in 3 double-blind, placebo-controlled, 12-week clinical trials. The 600-mg dose was studied in 2 of the 3 studies. Eleven out of 163 (7%) patients treated with 600 mg of HORIZANT discontinued treatment due to adverse reactions compared with 10 of the 245 (4%) patients who received placebo.
The most commonly observed adverse reactions (≥5% and at least 2 times the rate of placebo) in these trials for the 600-mg dose of HORIZANT were somnolence/sedation and dizziness (see Table 4). Table 4 lists treatment-emergent adverse reactions that occurred in ≥2% of patients with RLS treated with HORIZANT and numerically greater than placebo.
| Body System/Adverse Reaction | Placebo*
(N = 245) % | HORIZANT 600 mg/day† (N = 163) % | HORIZANT 1,200 mg/day‡ (N = 269) % |
|---|---|---|---|
|
|||
| Nervous system disorders | |||
| Somnolence/sedation | 6 | 20 | 27 |
| Dizziness | 4 | 13 | 22 |
| Headache | 11 | 12 | 15 |
| Gastrointestinal disorders | |||
| Nausea | 5 | 6 | 7 |
| Dry mouth | 2 | 3 | 4 |
| Flatulence | <1 | 3 | 2 |
| General disorders and administration site conditions | |||
| Fatigue | 4 | 6 | 7 |
| Irritability | 1 | 4 | 4 |
| Feeling drunk | 0 | 1 | 3 |
| Feeling abnormal | <1 | <1 | 3 |
| Peripheral edema | 1 | <1 | 3 |
| Metabolism and nutritional disorders | |||
| Weight increased | 2 | 2 | 3 |
| Increased appetite | <1 | 2 | 2 |
| Ear and labyrinth disorders | |||
| Vertigo | 0 | 1 | 3 |
| Psychiatric disorders | |||
| Depression | <1 | <1 | 3 |
| Libido decreased | <1 | <1 | 2 |
Adverse reactions reported in these three 12-week studies in <2% of patients treated with 600 mg of HORIZANT and numerically greater than placebo were balance disorder, blurred vision, disorientation, feeling drunk, lethargy, and vertigo.
The following adverse reactions were dose-related: somnolence/sedation, dizziness, feeling drunk, libido decreased, depression, headache, peripheral edema, and vertigo.
Postherpetic Neuralgia
The exposure to HORIZANT in 417 patients with PHN included 207 patients exposed for at least 3 months. Overall, the mean age of patients in the PHN studies ranged from 61 to 64 years of age across dose groups; the majority of patients were male (45% to 61%) and Caucasian (80% to 98%).
The safety of HORIZANT in doses ranging from 1,200 to 3,600 mg has been evaluated in 417 patients with PHN in 3 clinical studies. The principal efficacy study evaluating the efficacy and safety of HORIZANT in the management of PHN was a 12-week, double-blind, multicenter study comparing 1,200 mg/day, 2,400 mg/day and 3,600 mg/day to placebo. Six out of 107 (6%) patients treated with 1,200 mg of HORIZANT discontinued treatment due to adverse events compared with 12 of the 95 (13%) patients who received placebo.
The most commonly observed adverse reactions (≥10% and greater than placebo) in this trial for the 1,200 mg dose of HORIZANT were dizziness, somnolence, and headache (see Table 5). Table 5 lists treatment-emergent adverse reactions that occurred in ≥2% of patients with PHN treated with HORIZANT 1,200 mg/day and numerically greater than placebo.
| Body System/Adverse Reaction | Placebo (N = 95) % | HORIZANT 1,200 mg/day (N = 107) % | HORIZANT 2,400 mg/day (N = 82) % | HORIZANT 3,600 mg/day (N = 87) % |
|---|---|---|---|---|
| Nervous System | ||||
| Dizziness | 15 | 17 | 26 | 30 |
| Somnolence | 8 | 10 | 11 | 14 |
| Headache | 9 | 10 | 10 | 7 |
| Gastrointestinal disorders | ||||
| Nausea | 5 | 8 | 4 | 9 |
| General disorders and administration site conditions | ||||
| Fatigue/Asthenia | 1 | 6 | 4 | 10 |
| Peripheral edema | 0 | 6 | 7 | 6 |
| Psychiatric disorders | ||||
| Insomnia | 2 | 3 | 5 | 7 |
| Metabolism and nutritional disorders | ||||
| Weight increased | 1 | 3 | 5 | 5 |
| Eye disorders | ||||
| Blurred vision | 0 | 2 | 5 | 2 |
The following adverse reactions were also reported as ≥2% at 2,400 mg/day and/or 3,600 mg/day and appeared to be dose-related but were <2% at 1,200 mg/day: balance disorder, confusional state, depression, dry mouth, flatulence, increased appetite, irritability, and vertigo. Dizziness, somnolence, fatigue, and insomnia appeared to show a dose relationship.
6.2 Postmarketing Experience
The following adverse reactions have been reported in patients receiving gabapentin and have been identified during postapproval use of HORIZANT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure: breast enlargement, gynecomastia, elevated creatine kinase, bullous pemphigoid.
There are postmarketing reports of life-threatening or fatal respiratory depression in patients taking gabapentin with opioids or other CNS depressants, or in the setting of underlying respiratory impairment [see Warnings and Precautions (5.5)].
7. Drug Interactions
Gabapentin enacarbil is released faster from HORIZANT Extended-Release tablets in the presence of alcohol. Consumption of alcohol is not recommended when taking HORIZANT [see Clinical Pharmacology (12.3)].
Morphine: HORIZANT taken in conjunction with morphine causes increased somnolence/sedation, dizziness, and nausea when compared with either drug alone [see Clinical Pharmacology (12.3)].
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
There are no adequate data on the developmental risk associated with the use of HORIZANT in pregnant women. In nonclinical studies in rats and rabbits, administration of gabapentin enacarbil was developmentally toxic when administered to pregnant animals at doses and gabapentin exposures greater than those used clinically [see Data].
In the US general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
Data
Animal data
When pregnant rats were administered gabapentin enacarbil (oral doses of 200, 1,000, or 5,000 mg/kg/day) throughout the period of organogenesis, embryofetal mortality was increased at the 2 highest doses and fetal body weights were decreased at the high dose. The no-effect dose for embryofetal developmental toxicity in rats (200 mg/kg/day) represents approximately 2 times the gabapentin exposure associated with the maximum recommended human dose (MRHD) of 1,200 mg/day gabapentin enacarbil on an area under the curve (AUC) basis.
When pregnant rabbits were administered gabapentin enacarbil (oral doses of 200, 500, or 2,500 mg/kg/day) throughout the period of organogenesis, embryofetal mortality was increased and fetal body weights were decreased at the high dose. The no-effect dose for embryofetal developmental toxicity in rabbits (500 mg/kg/day) represents approximately 9 times the gabapentin exposure associated with the MRHD of 1,200 mg/day gabapentin enacarbil on an AUC basis.
When female rats were administered gabapentin enacarbil (oral doses of 200, 1,000, or 5,000 mg/kg/day) throughout the pregnancy and lactation periods, offspring growth and survival were decreased at the two highest doses. The no-effect dose for pre- and post-natal developmental toxicity in rats is approximately 2 times the MRHD on an AUC basis.
In reproductive and developmental studies of gabapentin, developmental toxicity was observed at all doses tested. Increased incidences of hydroureter and/or hydronephrosis were observed in rat offspring following treatment of pregnant animals in studies of fertility and general reproductive performance, embryofetal development, and peri- and post-natal development. Overall, a no-effect dose was not established. In mice, treatment of pregnant animals with gabapentin during the period of organogenesis resulted in delayed fetal skeletal ossification at all but the lowest dose tested. When pregnant rabbits were treated with gabapentin during the period of organogenesis, an increase in embryofetal mortality was observed at all doses of gabapentin tested.
In a published study, gabapentin (400 mg/kg/day) was administered by intraperitoneal injection to neonatal mice during the first postnatal week, a period of synaptogenesis in rodents (corresponding to the last trimester of pregnancy in humans). Gabapentin caused a marked decrease in neuronal synapse formation in brains of intact mice and abnormal neuronal synapse formation in a mouse model of synaptic repair. Gabapentin has been shown in vitro to interfere with activity of the α2δ subunit of voltage-activated calcium channels, a receptor involved in neuronal synaptogenesis. The clinical significance of these findings is unknown.
8.2 Lactation
Risk Summary
It is not known whether gabapentin derived from HORIZANT is secreted in human milk; however, gabapentin is secreted into human milk following oral administration of other gabapentin products. There are no data on the effects of gabapentin on the breastfed infant or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for HORIZANT and any potential adverse effects on the breastfed infant from HORIZANT or from the underlying maternal condition.
8.5 Geriatric Use
Of the 515 patients treated with HORIZANT in the 3 double-blind, placebo-controlled, 12-week clinical trials for RLS, 11% were 65 to 74 years of age and 1% were 75 years of age and older. Clinical trials of HORIZANT for the treatment of RLS did not include a sufficient number of patients 65 years and older to determine whether they respond differently from younger individuals.
In the 12-week, double-blind, placebo-controlled study of HORIZANT for the management of PHN (n = 276 patients treated with HORIZANT), 37% were 65 to 74 years of age and 13% were 75 years of age and older. The overall incidence of adverse events was comparable between the patients aged ≥18 to <65 years and ≥65 to <74 years. No overall differences in the safety and effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Gabapentin is known to be almost exclusively excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, the frequency of dosing may need to be adjusted based on calculated creatinine clearance in these patients [see Dosage and Administration (2.3)].
8.6 Renal Impairment
The dose of HORIZANT should be adjusted in patients with renal impairment [see Dosage and Administration (2.3), Clinical Pharmacology (12.3)].
9. Drug Abuse and Dependence
9.2 Abuse
Gabapentin does not exhibit affinity for benzodiazepine, opiate (mu, delta, or kappa), or cannabinoid 1 receptor sites. A small number of postmarketing cases report gabapentin misuse and abuse. These individuals were taking higher than recommended doses of gabapentin for unapproved uses. Most of the individuals described in these reports had a history of poly- substance abuse or used gabapentin to relieve symptoms of withdrawal from other substances.
When prescribing products that deliver gabapentin, carefully evaluate patients for a history of drug abuse and observe them for signs and symptoms of gabapentin misuse or abuse (e.g., development of tolerance, self-dose escalation, and drug-seeking behavior).
9.3 Dependence
There are rare postmarketing reports of individuals experiencing withdrawal symptoms shortly after discontinuing higher than recommended doses of gabapentin used to treat illnesses for which the drug is not approved. Such symptoms included agitation, disorientation, and confusion after suddenly discontinuing gabapentin that resolved after restarting gabapentin. Most of these individuals had a history of poly-substance abuse or used gabapentin to relieve symptoms of withdrawal from other substances. The dependence and abuse potential of gabapentin has not been evaluated in human studies.
10. Overdosage
10.1 Human Overdose Experience
The incidence of central nervous system adverse reactions, particularly dizziness and somnolence/sedation, is increased with HORIZANT doses greater than 600 mg daily.
Acute oral overdoses of gabapentin have been reported. Symptoms have included double vision, tremor, slurred speech, drowsiness, altered mental status, dizziness, lethargy, and diarrhea. Fatal respiratory depression has been reported with gabapentin overdose, alone and in combination with other CNS depressants.
10.2 Overdosage Management
In the event of an overdose, the patient should be treated supportively with appropriate monitoring as necessary. Gabapentin derived from gabapentin enacarbil can be removed from plasma by hemodialysis. The mean percentage of gabapentin recovered following hemodialysis in patients with end-stage renal disease was 29% (expressed as a proportion of the gabapentin released from HORIZANT).
Further management should be as clinically indicated or as recommended by a poison control center.
11. Horizant Description
HORIZANT (gabapentin enacarbil) is a prodrug of gabapentin. Gabapentin enacarbil is described as (1-{[({(1RS)-1-[(2-Methylpropanoyl)oxy]ethoxy}carbonyl)amino]methyl} cyclohexyl) acetic acid. It has a molecular formula of C16H27NO6 and a molecular weight of 329.39. It is a racemate and has the following structural formula:
Gabapentin enacarbil is a white to off-white crystalline solid with a melting onset of approximately 64°C and a solubility of 0.5 mg/mL in water and 10.2 mg/mL in phosphate buffer (pH 6.3).
HORIZANT is administered orally. Each HORIZANT Extended-Release Tablet contains 300 mg or 600 mg of gabapentin enacarbil and the following inactive ingredients: colloidal silicon dioxide, dibasic calcium phosphate dihydrate, glyceryl behenate, magnesium stearate, sodium lauryl sulfate, and talc.
12. Horizant - Clinical Pharmacology
12.1 Mechanism of Action
Gabapentin enacarbil is a prodrug of gabapentin and, accordingly, its therapeutic effects in RLS and PHN are attributable to gabapentin.
The precise mechanism by which gabapentin is efficacious in RLS and PHN is unknown.
The mechanism of action by which gabapentin is efficacious in PHN is unknown but in animal models of analgesia, gabapentin prevents allodynia (pain-related behavior in response to a normally innocuous stimulus) and hyperalgesia (exaggerated response to painful stimuli). Gabapentin prevents pain-related responses in several models of neuropathic pain in rats and mice (e.g., spinal nerve ligation models, spinal cord injury model, acute herpes zoster infection model). Gabapentin also decreases pain-related responses after peripheral inflammation (carrageenan footpad test, late phase of formalin test), but does not alter immediate pain-related behaviors (rat tail flick test, formalin footpad acute phase). The relevance of these models to human pain is not known.
Gabapentin is structurally related to the neurotransmitter gamma-aminobutyric acid (GABA) but has no effect on GABA binding, uptake, or degradation. Gabapentin enacarbil and gabapentin have been tested in radioligand binding assays, and neither exhibited affinity for a number of other common receptor, ion channel, or transporter proteins.
In vitro studies have shown that gabapentin binds with high affinity to the α2δ subunit of voltage-activated calcium channels; however, the relationship of this binding to the therapeutic effects of gabapentin enacarbil in RLS and PHN is unknown.
12.3 Pharmacokinetics
HORIZANT is an extended-release formulation of gabapentin enacarbil, a prodrug of gabapentin. HORIZANT provides approximately dose-proportional and extended exposure to gabapentin over the range 300 to 6,000 mg. HORIZANT and gabapentin are not interchangeable because the same daily dose of each results in different plasma concentrations of gabapentin.
For subjects with PHN taking HORIZANT 600 mg twice daily, the estimated steady state mean Cmax was 5.35 µg/mL, mean AUC24 was approximately 109 µg*hr/mL, mean Cmin was 3.63 µg/mL, and mean peak trough ratio was 1.5.
Absorption
The pathway for absorption of gabapentin enacarbil is believed to include active transport via a proton-linked monocarboxylate transporter, MCT-1. This transporter is expressed at high levels in the intestinal tract and is not saturated by administration of high doses of HORIZANT. Mean bioavailability of gabapentin (based on urinary recovery of gabapentin) for HORIZANT in the fed state is about 75%. Bioavailability under fasting conditions has been estimated by gabapentin urinary recovery to be 42% to 65%. In a food effect study, the exposure of gabapentin increased by 24%, 34%, and 44% with low, moderate, and high fat meals, respectively. The Tmax of gabapentin after administration of 600 mg of HORIZANT was 5.0 hours in fasted subjects and 7.3 hours in fed subjects. Steady state is reached in 2 days with daily administration.
Distribution
Plasma protein binding of gabapentin has been reported to be <3%. The apparent volume of distribution of gabapentin in subjects receiving HORIZANT is 76 L.
Metabolism
After oral administration, gabapentin enacarbil undergoes extensive first-pass hydrolysis by non-specific carboxylesterases primarily in enterocytes and to a lesser extent in the liver, to form gabapentin, carbon dioxide, acetaldehyde, and isobutyric acid. Levels of gabapentin enacarbil in blood are low and transient (≤2% of corresponding gabapentin plasma levels). Released gabapentin is not appreciably metabolized in humans. Neither gabapentin enacarbil nor gabapentin are substrates, inhibitors, or inducers of the major cytochrome P450 enzymes (CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4). Gabapentin enacarbil is neither a substrate nor an inhibitor of P-glycoprotein in vitro.
Elimination
Following hydrolysis of gabapentin enacarbil, the released gabapentin is excreted unchanged by the kidney. Gabapentin renal excretion is believed to involve a component of active secretion via an organic cation transporter (OCT2) present in the kidney. In a human pharmacokinetic study with immediate release 14C gabapentin enacarbil, mean recovery of total radioactivity in urine was 94%, with 5% of the radioactive dose recovered in feces.
Apparent oral clearance (CL/F) of gabapentin from plasma after dosing of HORIZANT with food ranged from 6.0 to 9.3 L/hr. Following oral dosing of HORIZANT, plasma clearance of gabapentin is approximately proportional to creatinine clearance. Renal clearance (CLr) of gabapentin ranged from 5 to 7 L/hr, regardless of food intake or food type. The elimination half-life (t½) of gabapentin ranges from 5.1 to 6.0 hours and is unaltered by dose or following multiple doses of HORIZANT.
Specific Populations
Race: In the population pharmacokinetic study, the majority (94%) of subjects in the clinical studies was Caucasian, and no single other race was greater than 4%; therefore, the effect of race could not be studied.
Gender: There are no clinically meaningful differences in pharmacokinetics of HORIZANT between male and female patients.
Geriatric Patients: There are no clinically significant differences in pharmacokinetics of HORIZANT between geriatric patients (≥65 years of age) and younger patients (18 to <65 years of age). However, the pharmacokinetics in geriatric patients may be affected by an age-related decline in renal function [see Use in Specific Populations (8.5)].
Renal Impairment: Gabapentin clearance after dosing with HORIZANT is approximately proportional to CrCl. Apparent oral clearance (CL/F) decreased in moderate (4.2 L/hr) and severe renal impairment patients (1.7 L/hr) compared with 6.0 to 9.3 L/hr in patients without renal impairment. Similarly, CLr was decreased to 3 and 1 L/hr in moderate and severe renal impairment patients, respectively, compared with 5 to 7 L/hr in non-renal impairment patients. Dosage reduction in patients with renal dysfunction not on dialysis is necessary.
Gabapentin is effectively removed from plasma by hemodialysis. The mean percentage of gabapentin recovered following hemodialysis in patients with end-stage renal disease was 29% (expressed as a proportion of the gabapentin released from HORIZANT). For patients with PHN on hemodialysis, dosage reduction is required [see Dosage and Administration (2.3)]. For patients with RLS on hemodialysis, treatment with HORIZANT is not recommended [see Dosage and Administration (2.3)].
Drug Interactions
Neither gabapentin enacarbil nor gabapentin are substrates, inhibitors, or inducers of the major cytochrome P450 enzymes. Gabapentin enacarbil is neither a substrate nor an inhibitor of P-glycoprotein in vitro.
Pharmacokinetic drug-drug interaction studies were conducted to examine the potential for an interaction of gabapentin enacarbil with cimetidine and naproxen. No significant pharmacokinetic interactions were observed. No clinically relevant pharmacokinetic interactions are expected between HORIZANT and other substrates of organic cation transporter type 2 (OCT2) and monocarboxylate transporter type 1 (MCT-1).
Ethanol: An in vitro dissolution study was conducted to evaluate the impact of ethanol (5, 10, 20, and 40%), on the extended-release characteristics of HORIZANT. The in vitro study showed that about 63% of the total gabapentin enacarbil dose was released at 1 hour at the highest alcohol level (40%), and about 43% of total drug was released at 1 hour with 5% alcohol. Ethanol causes a more rapid release of gabapentin enacarbil from the extended-release tablets that may increase the risk for adverse events associated with HORIZANT. Consumption of alcohol is not recommended when taking HORIZANT.
Cimetidine: Gabapentin released from HORIZANT is eliminated by renal clearance via OCT2. Cimetidine is a known substrate for this same elimination pathway. Coadministration of 1,200 mg of HORIZANT once daily with cimetidine 400 mg 4 times daily showed no effect on cimetidine exposure. There was an increase in AUC of gabapentin (24%) and a decrease in renal clearance of gabapentin (20%); these effects are not expected to be clinically relevant. No clinically relevant pharmacokinetic interactions are expected between HORIZANT and other substrates of OCT2.
Naproxen: The pathway for absorption of gabapentin enacarbil includes active transport via a proton-linked MCT-1. Coadministration of 1,200 mg of HORIZANT once daily with naproxen 500 mg twice daily, a known substrate of MCT-1, showed no effect on naproxen exposure or steady-state gabapentin Cmax and AUC. No clinically relevant pharmacokinetic interactions are expected between HORIZANT and other substrates of MCT-1.
Morphine: Administration of a single 600-mg dose of HORIZANT 2 hours after a single 60-mg dose of extended-release morphine sulfate in 18 subjects was associated with increased somnolence/sedation, dizziness, and nausea for the combination compared to HORIZANT or morphine alone as measured by the visual analog scale. No changes in Cmax and AUC of gabapentin, morphine or its active metabolite morphine-6-glucuronide were observed.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Oral (gavage) carcinogenicity studies were conducted in mice and rats.
In mice, gabapentin enacarbil was tested at doses of 500, 2,000, or 5,000 mg/kg/day for up to 104 weeks. There was no evidence of drug-related carcinogenicity. The highest dose tested is 16 times the MRHD of 1,200 mg/day, on a plasma AUC basis.
In rats, gabapentin enacarbil was tested at doses of 500, 2,000, or 5,000 mg/kg/day for up to 97 weeks in mid-dose males, 90 weeks in high-dose males, and 104 weeks in females. The plasma exposures (AUC) for gabapentin at these doses are approximately 4, 17, and 37 times, respectively, that in humans at the MRHD. Increases in the incidence of pancreatic acinar adenoma and carcinoma were found in mid-dose males and high-dose males and females.
In 2-year dietary carcinogenicity studies of gabapentin, no evidence of drug-related carcinogenicity was observed in mice treated at doses up to 2,000 mg/kg/day. In rats, increases in the incidence of pancreatic acinar cell adenoma and carcinoma were found in male rats receiving the highest dose (2,000 mg/kg), but not at doses of 250 or 1,000 mg/kg/day. At 1,000 mg/kg/day, the plasma AUC for gabapentin is estimated to be approximately 13 times that in humans at the MRHD.
Studies designed to investigate the mechanism of gabapentin-induced pancreatic carcinogenesis in rats indicate that gabapentin stimulates DNA synthesis in rat pancreatic acinar cells in vitro and thus may be acting as a tumor promoter by enhancing mitogenic activity. It is not known whether gabapentin has the ability to increase cell proliferation in other cell types or in other species, including human.
Mutagenesis
Gabapentin enacarbil was negative in in vitro bacterial reverse mutation (Ames) and in vivo rat micronucleus assays. In an in vitro human lymphocyte assay, there was an increase in the number of chromosomal aberrations with gabapentin enacarbil. This in vitro response was attributed to acetaldehyde released by hydrolysis of gabapentin enacarbil during the incubation period. Acetaldehyde is known to cause chromosome aberrations in vitro, but is readily metabolized in vivo. The small quantity of acetaldehyde formed from gabapentin enacarbil in vivo is rapidly cleared by normal metabolic activity.
Impairment of Fertility
Oral administration of gabapentin enacarbil (doses of 0, 200, 1,000, or 5,000 mg/kg/day) to male and female rats prior to and throughout mating and continuing in females up to day 7 of gestation resulted in no adverse effects on fertility. The highest dose tested is approximately 39 times the MRHD on an AUC basis.
14. Clinical Studies
14.1 Restless Legs Syndrome (RLS) 12-Week Pivotal Studies
The effectiveness of HORIZANT in the treatment of moderate-to-severe primary RLS was demonstrated in two 12-week clinical studies in adults diagnosed with RLS using the International Restless Legs Syndrome Study Group diagnostic criteria. Key diagnostic criteria for RLS are: an urge to move the legs usually accompanied or caused by uncomfortable and unpleasant leg sensations, symptoms begin or worsen during periods of rest or inactivity such as lying or sitting, symptoms are partially or totally relieved by movement such as walking or stretching at least as long as the activity continues, and symptoms are worse or occur only in the evening or night. Patients were required to have a total score of ≥15 on the International Restless Legs Syndrome (IRLS) Rating Scale at baseline. Patients with RLS secondary to other conditions (e.g., pregnancy, renal failure, iron deficiency anemia) were excluded. In study 1, patients were randomized to receive 1,200 mg of HORIZANT (N = 112) or placebo (N = 108) taken once daily at about 5 PM with food. In study 2, patients were randomized to receive 600 mg of HORIZANT (N = 114), 1,200 mg of HORIZANT (N = 111), or placebo (N = 96) taken once daily at about 5 PM with food.
Efficacy was evaluated using the IRLS Rating Scale and Clinical Global Impression of Improvement (CGI-I) scores. The IRLS Rating Scale contains 10 items designed to assess the severity of sensory and motor symptoms, sleep disturbance, daytime somnolence/sedation, and impact on activities of daily living and mood associated with RLS. The range of scores is 0 to 40, with 0 being absence of RLS symptoms and 40 the most severe symptoms. The CGI-I Scale allows the investigator to rate the patient's overall change in RLS symptoms since baseline, whether or not in the opinion of the investigator the change is related to study drug treatment. The change from baseline in the IRLS Rating Scale at Week 12 and the proportion of responders on the CGI-I Scale defined as a rating of "much improved" or "very much improved" at Week 12 were co-primary outcomes in these studies.
In these 2 studies, the mean age of patients studied was 50 years (range: 18 to 81 years); 59% of the patients were female. The racial distribution for these studies was as follows: Caucasian, 95%; black, 2%; and other, 3%.
Statistically significant differences (P<0.05) between the treatment groups receiving 600 and 1,200 mg of HORIZANT and the group receiving placebo were observed at Week 12 for both the mean change from baseline in the IRLS Scale total score and the proportion of responders ("much improved" or "very much improved") on the CGI-I Scale as described in Table 6.
| Week 12 | Study 1 | Study 2 | |||
|---|---|---|---|---|---|
| HORIZANT 1,200 mg (N = 112) | Placebo (N = 108) | HORIZANT 600 mg (N = 114) | HORIZANT 1,200 mg (N = 111) | Placebo (N = 96) |
|
|
|||||
| Mean Change in IRLS Score | -13.2 | -8.8 | -13.8 | -13.0 | -9.8 |
| Proportion of Responders* on CGI-I | 76% | 39% | 73% | 77% | 45% |
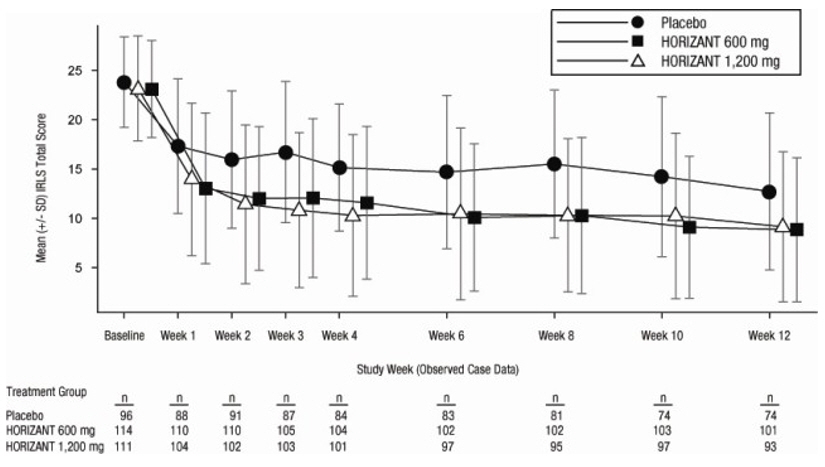
Figure 1 presents the improvement in mean IRLS Rating Scale total score in patients treated with placebo or 600 or 1,200 mg of HORIZANT over the 12 weeks of treatment in study 2.
Figure 1. Study 2, Mean (±SD) IRLS Rating Scale Total Score Over 12 Weeks (Observed Case Data, Modified Intent-To-Treat Population)
14.2 Postherpetic Neuralgia (PHN) 12-Week Study
The efficacy of HORIZANT for the management of postherpetic neuralgia was established in a multicenter, randomized, double-blind, parallel-group, placebo-controlled, 12- week study evaluating the efficacy, safety, and dose response of 3 maintenance doses of HORIZANT (1,200, 2,400, and 3,600 mg/day, with 107, 82, and 87 patients in each dosing group, respectively). Patients greater than 18 years of age with a documented medical diagnosis of PHN of at least three months duration were enrolled. To ensure that patients had significant pain, randomized patients were required to have a minimum baseline 24-hour average Pain Intensity Numerical Rating Scale (PI-NRS) intensity score of at least 4.0 on the 11-point numerical PI-NRS, ranging from 0 ("no pain") to 10 ("pain as bad as you can imagine").
In this study, a total of 276 patients received HORIZANT while 95 patients received placebo. Following a 1-week baseline period during which patients were screened for eligibility, patients began a 1-week up-titration period followed by a 12-week maintenance treatment period, and then a 1-week down-titration period.
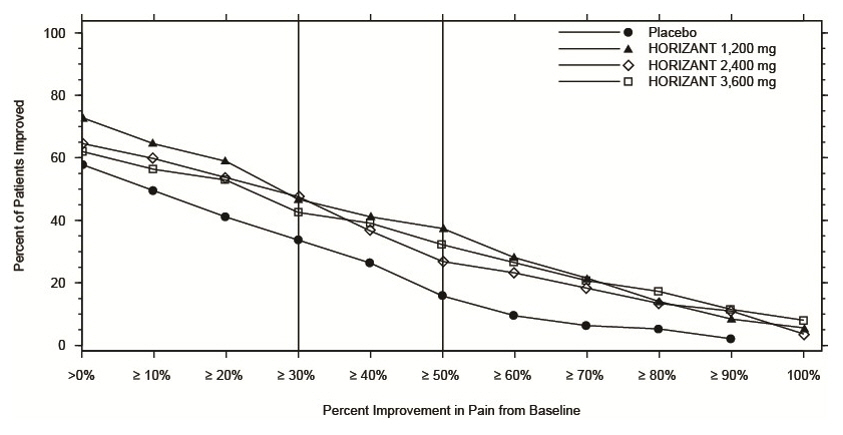
Treatment with HORIZANT statistically significantly improved the mean pain score and increased the proportion of patients with at least a 50% reduction in pain score from baseline at all doses tested. A benefit over placebo was observed for all 3 doses of HORIZANT as early as Week 1 and maintained to the end of treatment. Additional benefit of using doses of greater than 1,200 mg a day was not demonstrated.
For various degrees of improvement in pain from baseline to end of maintenance treatment, Figure 2 shows the fraction of patients achieving that degree of improvement. The figure is cumulative, so that patients whose change from baseline is, for example, 50%, are also included at every level of improvement below 50%. Patients who did not complete the study were assigned 0% improvement.
Figure 2. Percent of Patients Achieving Various Levels of Improvement in Pain Intensity
14.3 Effects on Driving
Driving performance was assessed in a three way crossover study in healthy volunteers (mean age 36 years). Subjects were dosed at approximately 5 pm with HORIZANT 600 mg (for five days), diphenhydramine 50 mg (1 dose), and placebo (for five days). After the last dose, driving was evaluated on a computer-based simulation for 1 hour in the evening approximately 2 to 4 hours after dosing (7 to 9 pm), in the morning after dosing (7 to 9 am), and at midday the day after dosing (11 am to 1 pm). The primary endpoint of the study was lane position variability. There was no difference in change from baseline in lane position variability for HORIZANT compared to placebo at any of the simulated driving timepoints. Secondary measures included speed variability and the occurrence of simulated crashes. Subjects in this study experienced simulated crashes as described in Table 7. At the times that simulated crashes occurred, there was an increase in average speed variability in the HORIZANT- and diphenhydramine-treated groups that was most notable in patients who experienced simulated crashes, but no increases in lane position variability. Later time points post-dosing or the effects of driving after more than five days of dosing with HORIZANT were not evaluated.
| Simulated Driving Timepoint and Hours Post Dose | Baseline N = 36 n (%) | Placebo N = 36 n (%) | HORIZANT 600 mg N = 35 n (%) | Diphenhydramine 50 mg N = 36 n (%) |
|---|---|---|---|---|
| Day 5
Evening (7 to 9 pm) 2 to 4 hours post dose | 0 (0) | 0 (0) | 0 (0) | 3 (9) |
| Day 6
Morning (7 to 9 am) 14 to 16 hours post dose | 2 (6) | 1 (3) | 1 (3) | 0 (0) |
| Day 6
Midday (11 am to 1 pm) 18 to 20 hours post dose | 1 (3) | 0 (0) | 3 (9) | 3 (8) |
The results of a separate 2-week driving simulation study in patients (mean age 47 years) with moderate-to-severe primary RLS showed that once daily doses of 1,200 mg and 1,800 mg of HORIZANT significantly impaired simulated driving performance based on lane position variability. An increased number of simulated crashes were reported in patients tested near Tmax after receiving 1,200 mg or 1,800 mg of HORIZANT compared to patients treated with diphenhydramine 50 mg. In addition, patients receiving 1,200 mg of HORIZANT experienced an increased number of simulated crashes at 14 to 16 hours after dosing compared with placebo, diphenhydramine, and 1,800 mg of HORIZANT.
The design limitations of these two studies do not permit inference regarding dose response relationship or the duration of the effect HORIZANT has on driving in patients with RLS.
The results of a separate driving simulation study comparing untreated RLS patients and healthy subjects showed no difference in lane position variability but an increase in speed variability associated with a greater number of simulated crashes in RLS patients relative to healthy subjects, which may indicate impaired driving in RLS patients in the absence of medication.
16. How is Horizant supplied
HORIZANT Extended-Release Tablets containing 300 mg of gabapentin enacarbil are white to off-white, with occasional black/grey spots, oval-shaped tablets debossed with "GS TF7".
HORIZANT Extended-Release Tablets containing 600 mg of gabapentin enacarbil are white to off-white, with occasional black/grey spots, oval-shaped tablets debossed with "GS LFG". They are supplied as follows:
- 300 mg: NDC 53451-0103-1: Bottles of 30
- 600 mg: NDC 53451-0101-1: Bottles of 30
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Effects on Driving
Patients should be told that HORIZANT may cause a significant driving impairment. Accordingly, they should be advised not to drive a car until they have gained sufficient experience on HORIZANT to assess whether HORIZANT impairs their ability to drive, although patients' ability to determine their level of impairment can be unreliable. Patients should be told that it is not known how long this effect lasts [see Warnings and Precautions (5.1)].
Somnolence/Sedation and Dizziness
Patients should be told that HORIZANT can cause significant somnolence and dizziness. This typically resolves within several weeks of initiating treatment. Accordingly, they should be told not to operate dangerous machinery until they have gained sufficient experience on HORIZANT to assess whether HORIZANT impairs their ability to operate dangerous machinery safely [see Warnings and Precautions (5.2)].
Suicidal Behavior and Ideation
Patients, their caregivers, and families should be counseled that HORIZANT may increase the risk of suicidal thoughts and behavior, and should be advised of the need to be alert for the emergence or worsening of symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm [see Warnings and Precautions (5.4)].
Behaviors of concern should be reported immediately to healthcare providers.
Respiratory Depression
Inform patients about the risk of respiratory depression. Include information that the risk is greatest for those using concomitant CNS depressants (such as opioid analgesics), or those with concurrent respiratory impairment. Teach patients how to recognize respiratory depression and advise them to seek medical attention immediately if it occurs [see Warnings and Precautions (5.5)].
Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS)/Multiorgan Hypersensitivity
Patients should be instructed that multiorgan hypersensitivity reactions may occur with HORIZANT. Patients should contact their physician immediately if they experience any signs or symptoms of these conditions [see Warnings and Precautions (5.5)].
Lack of Interchangeability With Gabapentin
Patients should be advised that doses of HORIZANT and other gabapentin products are not interchangeable [see Warnings and Precautions (5.3)].
Dosing Instructions [see Dosage and Administration (2)]
- Instruct patients to take HORIZANT only as prescribed.
- Instruct patients to swallow tablets whole and do not cut, crush, or chew tablets.
- Instruct patients to take HORIZANT with food.
- For Restless Legs Syndrome, 600 mg HORIZANT should be taken once daily at about 5 PM. If the dose is not taken at the recommended time, the patient should take the next dose at about 5 PM the following day.
- For Postherpetic Neuralgia, the starting dose is 600 mg HORIZANT in the morning for 3 days. Starting on day 4, 600 mg HORIZANT should be taken twice daily. If the dose is not taken at the recommended time, the next dose should be taken at the time of next scheduled dose.
- Instruct patients about how to discontinue HORIZANT.
Alcohol
Advise patients to avoid alcohol when taking HORIZANT [see Drug Interactions (7), Clinical Pharmacology (12.3)].
HORIZANT is a registered trademark of Azurity Pharmaceuticals, Inc.
Manufactured for:
Azurity Pharmaceuticals, Inc.
Woburn, MA 01801
Azurity Pharmaceuticals, Inc. All rights reserved.
HZT-PI-04
Medication Guide
HORIZANT® (ho-ri' zant) (gabapentin
enacarbil) Extended-Release Tablets
Read this Medication Guide before you start taking HORIZANT and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment.
What is the most important information I should know about HORIZANT?
HORIZANT can cause serious side effects:
- 1.
- Do not drive after taking your dose of HORIZANT until you know how HORIZANT affects you, including the morning after you take your dose. Do not operate heavy machinery or do other dangerous activities until you know how HORIZANT affects you. HORIZANT can cause sleepiness, dizziness, slow thinking, and can affect your coordination. Ask your healthcare provider when it would be okay to do these activities.
- 2.
-
HORIZANT may cause suicidal thoughts or actions in a very small number of people, about 1 in 500.
Call a healthcare provider right away if you have any of these symptoms, especially if they are new, worse, or worry you:- thoughts about suicide or dying
- attempt to commit suicide
- new or worse depression
- new or worse anxiety
- feeling agitated
- new or worse restlessness
- panic attacks
- new or worse trouble sleeping (insomnia)
- new or worse irritability
- acting aggressive, being angry, or violent
- acting on dangerous impulses
- an extreme increase in activity and talking (mania)
- other unusual changes in behavior or mood
How can I watch for early symptoms of suicidal thoughts and actions?- Pay attention to any changes, especially sudden changes, in mood, behaviors, thoughts, or feelings.
- Keep all follow-up visits with your healthcare provider as scheduled.
- Call your healthcare provider between visits as needed, especially if you are worried about symptoms.
Do not stop HORIZANT without first talking to a healthcare provider. Suicidal thoughts or actions can be caused by things other than medicines. If you have suicidal thoughts or actions, your healthcare provider may check for other causes. - 3.
-
HORIZANT may cause a serious or life-threatening allergic reaction that may affect your skin or other parts of your body such as your liver or blood cells. You may or may not have rash with these types of reactions. Call a healthcare provider right away if you have any of the following symptoms:
- skin rash
- hives
- fever
- swollen glands that do not go away
- swelling of your lips or tongue
- yellowing of your skin or eyes
- unusual bruising or bleeding
- severe fatigue or weakness
- unexpected, severe muscle pain
- frequent infections
These symptoms may be the first signs of a serious reaction. A healthcare provider should examine you to decide if you should continue taking HORIZANT. - 4.
- Serious breathing problems. Serious breathing problems can occur when HORIZANT is taken with other medicines that can cause severe sleepiness or decreased awareness, or when it is taken by someone who already has breathing problems. Watch for increased sleepiness or decreased breathing when starting HORIZANT or when the dose is increased. Get help right away if breathing problems occur.
What is HORIZANT?
HORIZANT is a prescription medicine used to treat adults with:
- moderate-to-severe primary Restless Legs Syndrome (RLS).
- pain from damaged nerves (postherpetic pain) that follows healing of shingles (a painful rash that comes after a herpes zoster infection).
HORIZANT is not for people with RLS who need to sleep during the daytime and need to stay awake at night.
HORIZANT is not the same medicine as gabapentin (for example, NEURONTIN® or GRALISE®) and should not be used in its place.
It is not known if HORIZANT is safe and effective in children.
What should I tell my healthcare provider before taking HORIZANT?
Before taking HORIZANT, tell your healthcare provider if you:
- have or have had kidney problems or are on hemodialysis.
- have or have had depression, mood problems, or suicidal thoughts or behavior.
- have or have had seizures.
- have a history of drug abuse.
- have breathing problems.
- have any other medical conditions.
- are pregnant or plan to become pregnant.
- It is not known if HORIZANT will harm your unborn baby. Talk to your healthcare provider if you are pregnant or plan to become pregnant while taking HORIZANT. You and your healthcare provider will decide if you should take HORIZANT while you are pregnant.
- are breastfeeding or plan to breastfeed. Your body turns HORIZANT into another drug (gabapentin) that passes into your milk. It is not known if this can harm your baby. You and your healthcare provider should decide if you will take HORIZANT or breastfeed.
- drink alcohol.
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements. Especially tell your healthcare provider if you take any opioid pain medicine (such as oxycodone), any medicines for anxiety (such as lorazepam) or insomnia (such as zolpidem), or any medicines that make you sleepy.
You may have a higher chance for dizziness, sleepiness, or breathing problems if these medicines are taken with HORIZANT.
Know the medicines you take. Keep a list of them and show it to your healthcare provider and pharmacist when you get a new medicine.
How should I take HORIZANT?
- Take HORIZANT exactly as your healthcare provider tells you to take it. Your healthcare provider will tell you how much HORIZANT to take and when to take it.
- Take HORIZANT tablets whole. Do not cut, crush, or chew your tablet.
- Take HORIZANT tablets with food.
- Do not stop taking HORIZANT without talking to your healthcare provider first. If you stop taking HORIZANT suddenly, you may develop side effects.
- If you forget to take your medicine at the time recommended by your healthcare provider, just skip the missed dose. Take the next dose at your regular time. Do not take 2 doses at one time.
- If you take too much HORIZANT, call your healthcare provider or go to the nearest hospital emergency room right away.
What should I avoid while taking HORIZANT?
- Do not take other medicines that make you sleepy or dizzy while taking HORIZANT without first talking with your healthcare provider. Taking HORIZANT with medicines that cause sleepiness or dizziness may make your sleepiness or dizziness worse.
- Do not take other gabapentin drugs (for example, NEURONTIN or GRALISE) while you take HORIZANT.
- Do not consume alcohol when taking HORIZANT.
What are the possible side effects of HORIZANT?
The most common side effects of HORIZANT include:
- sleepiness
- dizziness
- headache
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of HORIZANT. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store HORIZANT?
- Store HORIZANT between 59° and 86°F (15° and 30°C).
- Keep HORIZANT dry and away from moisture.
- Keep HORIZANT tightly closed in the bottle provided to you. Do not remove any moisture control packs that may come in the bottle.
Keep HORIZANT and all medicines out of the reach of children.
General Information about the safe and effective use of HORIZANT
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use HORIZANT for a condition for which it was not prescribed. Do not give HORIZANT to other people, even if they have the same symptoms that you have. It may harm them.
This Medication Guide summarizes the most important information about HORIZANT. If you would like more information, talk with your healthcare provider.
You can ask your healthcare provider or pharmacist for information about HORIZANT that was written for healthcare professionals.
For more information about HORIZANT, go to www.HORIZANT.com or call 1-800-461-7449.
What are the ingredients in HORIZANT?
Active ingredients: gabapentin enacarbil
Inactive ingredients: Both the 300 mg and 600 mg tablets contain colloidal silicon dioxide, dibasic calcium phosphate dihydrate, glyceryl behenate, magnesium stearate, sodium lauryl sulfate, and talc.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Manufactured for:
Azurity Pharmaceuticals, Inc.
Woburn, MA 01801
Revised: 8/2022
HORIZANT is a registered trademark of Azurity Pharmaceuticals, Inc. The other brands listed are trademarks of their respective owners and are not trademarks of Azurity Pharmaceuticals, Inc. The makers of these brands are not affiliated with and do not endorse Azurity Pharmaceuticals, Inc. or its products.
Azurity Pharmaceuticals, Inc. All rights reserved.
HZT-MG-02
| HORIZANT
gabapentin enacarbil tablet, extended release |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| HORIZANT
gabapentin enacarbil tablet, extended release |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Azurity Pharmaceuticals, Inc. (formerly Arbor Pharmaceuticals) (117505635) |
Frequently asked questions
More about Horizant (gabapentin enacarbil)
- Check interactions
- Compare alternatives
- Pricing & coupons
- Reviews (37)
- Drug images
- Side effects
- Dosage information
- During pregnancy
- FDA approval history
- Drug class: gamma-aminobutyric acid analogs
